Tetanus: Background, Pathophysiology, Etiology
- ️Invalid Date
Overview
Background
Tetanus is characterized by an acute onset of hypertonia, painful muscular contractions (usually of the muscles of the jaw and neck), and generalized muscle spasms without other apparent medical causes. Despite widespread immunization of infants and children since the 1940s, tetanus still occurs in the United States. [1] Tetanus primarily affects older adults because of their higher rate of being unvaccinated or inadequately vaccinated. [2] The image below illustrates tetanus cases in the United States from 1947-2023.
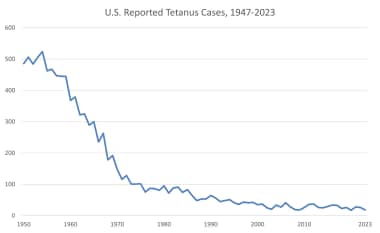
Reported number of tetanus cases in the United States from 1947-2023. Image from National Notifiable Disease Surveillance System (NNDSS), Centers for Disease Control and Prevention (CDC).
Tetanus may be categorized into the following 4 clinical types [1] :
-
Generalized tetanus
-
Localized tetanus
-
Cephalic tetanus
-
Neonatal tetanus
Approximately 50-75% of patients with generalized tetanus present with trismus (“lockjaw”), which is the inability to open the mouth secondary to masseter muscle spasm. Nuchal rigidity and dysphagia also are early complaints that cause risus sardonicus, the scornful smile of tetanus, resulting from facial muscle involvement. [3, 4]
As the disease progresses, patients have generalized muscle rigidity with intermittent reflex spasms in response to stimuli (eg, noise, touch). Tonic contractions cause opisthotonos (ie, flexion and adduction of the arms, clenching of the fists, and extension of the lower extremities). During these episodes, patients have an intact sensorium and feel severe pain. The spasms can cause fractures, tendon ruptures, and acute respiratory failure.
Patients with localized tetanus present with persistent rigidity in the muscle group close to the injury site. [1] The muscular rigidity is caused by a dysfunction in the interneurons that inhibit the alpha motor neurons of the affected muscles. No further central nervous system (CNS) involvement occurs in this form, and mortality is very low.
Cephalic tetanus is uncommon and usually occurs after head trauma or otitis media. Patients with this form present with cranial nerve (CN) palsies. The infection may be localized or may become generalized. [5]
Neonatal tetanus (tetanus neonatorum) is a major cause of infant mortality in underdeveloped countries but is rare in the United States. Infection results from umbilical cord contamination during unsanitary delivery, coupled with a lack of maternal immunization. At the end of the first week of life, infected infants become irritable, feed poorly, and develop rigidity with spasms. Neonatal tetanus has a very poor prognosis. [6, 7]
Although tetanus is quite rare, early diagnosis and intervention are lifesaving. Prevention is the ultimate management strategy for tetanus.
![]()
Pathophysiology
Clostridium tetani is an obligate, anaerobic, motile, gram-positive bacillus. [1] It is nonencapsulated and forms spores that are resistant to heat, desiccation, and disinfectants. Since the colorless spores are located at one end of the bacillus, they cause the organism to resemble a turkey leg. They are found in soil, house dust, animal intestines, and human feces. Spores can persist in normal tissue for months to years.
To germinate, the spores require specific anaerobic conditions, [8] such as wounds with low oxidation-reduction potential (eg, dead or devitalized tissue, foreign body, active infection). Under these conditions, upon germination, they may release their toxin. Infection by C tetani results in a benign appearance at the portal of entry because of the inability of the organism to evoke an inflammatory reaction unless coinfection with other organisms develops.
When the proper anaerobic conditions are present, the spores germinate and produce the following 2 toxins:
-
Tetanolysin – This substance is a hemolysin with no recognized pathologic activity
-
Tetanospasmin – This toxin is responsible for the clinical manifestations of tetanus [9] ; by weight, it is one of the most potent toxins known, with an estimated minimum lethal dose of 2.5 ng/kg body weight
Tetanospasmin is synthesized as a 150-kd protein consisting of a 100-kd heavy chain and a 50-kd light chain joined by a disulfide bond. [10] The heavy chain mediates binding of tetanospasmin to the presynaptic motor neuron and also creates a pore for the entry of the light chain into the cytosol. The light chain is a zinc-dependent protease that cleaves synaptobrevin. [1]
After the light chain enters the motor neuron, it travels by retrograde axonal transport from the contaminated site to the spinal cord in 2-14 days. When the toxin reaches the spinal cord, it enters central inhibitory neurons. The light chain cleaves the protein synaptobrevin, which is integral to the binding of neurotransmitter containing vesicles to the cell membrane.
As a result, gamma-aminobutyric acid (GABA)-containing and glycine-containing vesicles are not released, and there is a loss of inhibitory action on motor and autonomic neurons. [11] With this loss of central inhibition, there is autonomic hyperactivity as well as uncontrolled muscle contractions (spasms) in response to normal stimuli such as noises or lights.
Once the toxin becomes fixed to neurons, it cannot be neutralized with antitoxin. Recovery of nerve function from tetanus toxins requires sprouting of new nerve terminals and formation of new synapses.
Localized tetanus develops when only the nerves supplying the affected muscle are involved. Generalized tetanus develops when the toxin released at the wound spreads through the lymphatics and blood to multiple nerve terminals. The blood-brain barrier prevents direct entry of toxin to the CNS.
![]()
Etiology
Tetanus is caused by the active toxin-producing bacillus form of Clostridium tetani. Spores of C tetani are ubiquitous in the environment and can survive for years. [12] These spores are resistant to many forms of decontamination, but can convert to tetanus bacilli under the appropriate anaerobic conditions, at which point they produce tetanus toxins. Infection most commonly occurs due to wound contamination with spores, even from wounds where medical attention was not deemed necessary. [9] Cases have been documented without obvious wounds of sites for infection. Childbirth is a significant cause of tetanus infection in the developing world. [12] Moreover, injection drug use has been linked to disease clusters in the United States. [13] Chronic wounds, such as venous or diabetic foot ulcers, also have been associated with cases of tetanus. [14]
Underimmunization is an important cause of tetanus. [2] Tetanus affects nonimmunized persons, partially immunized persons, or fully immunized individuals who do not maintain adequate immunity with periodic booster doses. Only 12-14% of patients with tetanus in the United States have received a primary series of tetanus toxoid. During 2001-2008, 10% of all patients with tetanus were known to be current with tetanus immunization, with only 1 death among this group. Surveillance data from 1998-2000 revealed the following [13] :
-
In 73% of patients with tetanus in the United States, tetanus occurred after an acute injury, including puncture wounds (50%), lacerations (33%), and abrasions (9%)
-
Stepping on a nail accounted for 32% of the puncture wounds
-
Tetanus was found to occur in burn victims; in patients receiving intramuscular injections; in persons obtaining a tattoo; and in persons with frostbite, dental infections (eg, periodontal abscesses), penetrating eye injuries, and umbilical stump infections
-
Other reported risk factors included diabetes, chronic wounds (eg, skin ulcers, abscesses, or gangrene), parenteral drug abuse, and recent surgery (4% of US cases)
-
During 1998-2000, 12% of patients with tetanus in the United States had diabetes (with mortality, 31%), compared with 2% during 1995-1997; of these patients, 69% had acute injuries and 25% had gangrene or a diabetic ulcer
-
The median time interval between surgery and onset of tetanus was 7 days
-
Tetanus was reported after tooth extractions, root canal therapy, and intraoral soft tissue trauma
Worldwide risk factors for neonatal tetanus include the following [12] :
-
Use of inadequately-sterilized instruments or contaminated dressings
-
Unvaccinated mother
-
Lack of hand cleansing by provider prior to delivery
Immunity from tetanus decreases with advancing age. [15] Serologic testing for immunity has revealed a low level among elderly individuals in the United States. Approximately 50% of adults older than 50 years are nonimmune because they never were vaccinated or do not receive appropriate booster doses. The prevalence of immunity to tetanus in the United States exceeds 80% for persons aged 6-39 years but is only 28% for those older than 70 years.
![]()
Epidemiology
United States statistics
Because of the widespread use of tetanus immunizations, the reported incidence of tetanus in the United States has declined substantially since the mid 1940s. [16]
From 2001-2008, 233 cases of tetanus were reported in the United States, a 95% reduction since 1947. Deaths from the disease had decreased by 99% since that year. The case mortality rate was 13.2%. Tetanus cases among Hispanic individuals were approximately twice that among non-Hispanic persons, attributed to an increased rate of injection drug use among Hispanic patients. In the group of patients with known vaccination status, 40.2% had received no doses of tetanus toxoid; 15.4% of 195 patients had diabetes; and 15.3% of 176 were intravenous drug users. In the 51 individuals with an acute wound in whom adequate information was available, 96.1% had not received appropriate prophylaxis. [2]
By November 2024, 30 tetanus cases were reported in the United States via the National Notifiable Diseases Surveillance System for the calendar year, up from 15 total cases reported in 2023 (NNDSS). [17]
All 50 states require that children be vaccinated before being admitted to public schools. More than 96% of children have received 3 or more diphtheria and tetanus toxoids plus pertussis (DTP) vaccinations by the time they begin school. [18]
In 2022, vaccination uptake by age 14 years among adolescents born in 2008 continued to fall behind that of earlier birth cohorts and differed according to sociodemographic factors and access to healthcare compared with that among earlier birth cohorts. [19]
Vaccination uptake by age 13 years among those born in 2009 was similar to coverage estimates reported before the COVID-19 pandemic.
Among individuals aged 13-17 years, 2022 vaccination coverage levels were similar to 2021 levels. Coverage with at least 1 dose of tetanus, diphtheria, and acellular pertussis vaccine and at least 1 dose meningococcal conjugate vaccine was high and stable (around 90%). Healthcare providers should review adolescent vaccination records, especially those of adolescents born in 2008 as well as children and adolescents who are eligible for the Vaccines for Children program, to ensure all recommended vaccines are current.
Heroin users, particularly those who inject themselves subcutaneously, appear to be at high risk for tetanus. Quinine is used to dilute heroin and may support the growth of C tetani. [20] The incidence of tetanus in people who use injection drugs increased 7.4% between 1991 and 1997, from 3.6% of all cases in 1991-1994 to 11% in 1995-1997. Injection drug users accounted for 15% of US tetanus cases from 1998 to 2000 (see the image below). [13] Of the 19 people who used injection drugs and contracted tetanus in 1998-2000, only 1 reported an acute injury.
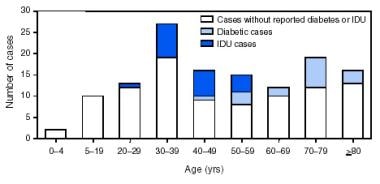
Image from "Number of Tetanus Cases Reported Among Persons With Diabetes or Injection-Drug Use (IDU), by Age Group." Pascual FB, McGinley EL, Zanardi LR, et al: Tetanus surveillance—United States, 1998−2000. MMWR Surveill Summ. 2003 Jun 20;52(3):1-8.
From 1998-2000, 81% of cases in the United States were generalized tetanus, 17% were localized, and 2% were cephalic; 1 case of neonatal tetanus was reported.
The CDC has not published a tetanus surveillance summary for the United States since 2008, but continues to publish the number of reported cases by state through the National Notifiable Diseases Surveillance System.
International statistics
C tetani is found worldwide in soil, on inanimate objects, in animal feces, and, occasionally, in human feces. Tetanus is predominantly a disease of underdeveloped countries. It is common in areas where soil is cultivated, in rural areas, in warm climates, during summer months, and among males. In countries without a comprehensive immunization program, tetanus predominantly develops in neonates and young children. [21, 22]
From 1990 to 2019, the incidence and death rate of tetanus fell significantly globally. [23]
Developed nations have incidences of tetanus similar to those observed in the United States. For instance, only 126 cases of tetanus were reported in England and Wales from 1984-1992. [24] More recently, the UK reported only 4 cases of tetanus in England during 2022, down from 11 cases the previous year. [25]
Although tetanus affects all ages, the highest prevalence is in newborns and young people. [26] The global burden of disease has fallen significantly since approximately 1990. [23] Incidence has decreased from an estimated 615,000 cases globally in 1990 to about 74,000 in 2019. Additionally, annual deaths from tetanus fell from 275,000 to 35,000 in this same time period. Neonatal tetanus accounted for half of all cases of tetanus and in some areas was the predominant cause of neonatal mortality, with close to 100% case fatality rates depending on regional access to care. Since 2000, global rates of neonatal tetanus have declined 89%, although disruption of vaccination efforts during the COVID-19 pandemic has led to increased disease incidence in many countries. [27]
Age-related demographics
Neonatal tetanus is rare in developed countries while accounting for a large burden of disease in resource-poor areas. [23]
The risk for development of tetanus and for the most severe form of the disease in developed countries is highest in the elderly population. In the United States from 2001-2008, the incidence rate among patients aged 65 years or older was approximately 0.23 cases per 1 million population vs 0.08 cases per 1 million population for those younger than 65 years. [2] Moreover, the relative risk for fatal disease was about five times higher in patients older than 65 compared with those under 65 years. Patient older than 65 years accounted for 77% of deaths during this period.
Sex-related demographics
Tetanus affects both sexes. No overall predilection by sex has been reported, except to the extent that males may have more soil exposure in some cultures. In the United States from 1998 to 2000, the incidence of tetanus was 2.8 times higher in males aged 59 years and younger than in females in the same age range. [13]
A difference in the levels of tetanus immunity exists between the sexes, with men being twice as likely to possess protective levels of antibodies compared with women. [15] This is speculated to be because of additional vaccinations administered during military service or professional activities.
Race-related demographics
Tetanus affects all races. From 2001-2008, the incidence of tetanus in the United States was almost twice as high among Hispanic individuals compared with non-Hispanic persons (0.13 vs 0.07 cases per million population). Exclusion of patients with injection drug use showed nearly equal incidences at 0.08 vs 0.07 cases per million populations among Hispanics and non-Hispanics, respectively. Incidence also was similar among other identified racial groups including White Americans (0.08 per million population), African Americans (0.07), American Indian/Alaska natives (0.09), and Asian/Pacific Islanders (0.07). [2]
![]()
Prognosis
The prognosis is dependent on incubation period, the time from spore inoculation to first symptom, and the time from first symptom to first tetanic spasm. [1] The following statements typically hold true [1] :
-
In general, shorter intervals indicate more severe tetanus and a poorer prognosis
-
Patients usually survive tetanus and return to their predisease state of health
-
Recovery is slow and usually occurs over 2-4 months
-
Some patients remain hypotonic
-
Clinical tetanus does not produce a state of immunity; therefore, patients who survive the disease require active immunization with tetanus toxoid to prevent a recurrence
A rating scale has been developed for assessing the severity of tetanus and determining the prognosis. On this scale, 1 point is given for each of the following [1] :
-
Incubation period shorter than 7 days
-
Period of onset shorter than 48 hours
-
Tetanus acquired from burns, surgical wounds, compound fractures, septic abortion, umbilical stump, or intramuscular injection
-
Narcotic addiction
-
Generalized tetanus
-
Temperature higher than 104°F (40°C)
-
Tachycardia exceeding 120 beats/min (150 beats/min in neonates)
The total score indicates disease severity and prognosis as follows:
-
0 or 1 – Mild tetanus; mortality below 10%
-
2 or 3 – Moderate tetanus; mortality of 10-20%
-
4 – Severe tetanus; mortality of 20-40%
-
5 or 6 – Very severe tetanus; mortality above 50%
Cephalic tetanus always is severe or very severe. Neonatal tetanus always is very severe.
The case-fatality ratio in the United States was 91% in 1947, 21-31% from 1982 to 1990, 11% from 1995 to 1997, 18% from 1998 to 2000, and 13.2% from 2001-2008. [2, 13] Mortality in mild and moderate tetanus is approximately 6%; for severe tetanus, it may be as high as 60%. Mortality in the United States resulting from generalized tetanus is 30% overall, 52% in patients older than 60 years, and 13% in patients younger than 60 years.
Mortality is substantially higher for people older than 65 years, with approximately 5 times the relative risk for death compared to cases in patients younger than 65 years. [2] From 1998 to 2000, 75% of the deaths in the United States were in patients older than 60 years. [13] In addition, mortality is notably higher for people who require mechanical ventilation (30%) than for those who do not (4%).
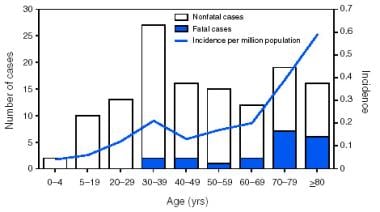
Image from "Number of Tetanus Cases Reported, Average Annual Incidence Rates, and Survival Status of Patients, by Age Group." Pascual FB, McGinley EL, Zanardi LR, et al: Tetanus surveillance—United States, 1998−2000. MMWR Surveill Summ. 2003 Jun 20;52(3):1-8.
Clinical tetanus is less severe among patients who have received a primary series of tetanus toxoid sometime during their life than among patients who are inadequately vaccinated or unvaccinated. [13] Mortality in the United States is 7% for individuals who had previously received at least 1 dose of tetanus vaccine versus 31% of those who were unvaccinated. [2]
![]()
Patient Education
The importance of childhood immunizations and boosters in adulthood must be stressed. Midwives and birth attendants in developing and underdeveloped countries should be given training in aseptic birthing procedures. The basics of wound care and first aid should be widely taught. Early recognition of symptoms and signs of localized tetanus and timely access to medical care are essential.
![]()
[Guideline] CDC. Clinical Overview of Tetanus. Centers for Disease Control and Prevention. Available at https://www.cdc.gov/tetanus/hcp/clinical-overview. August 15, 2024; Accessed: December 15, 2024.
Tetanus surveillance --- United States, 2001-2008. MMWR Morb Mortal Wkly Rep. 2011 Apr 1. 60(12):365-9. [QxMD MEDLINE Link]. [Full Text].
Pearce JM. Notes on tetanus (lockjaw). J Neurol Neurosurg Psychiatry. 1996 Mar. 60(3):332. [QxMD MEDLINE Link]. [Full Text].
Weinstein L. Tetanus. N Engl J Med. 1973 Dec 13. 289 (24):1293-6. [QxMD MEDLINE Link]. [Full Text].
Blain Am Tejpratap SP, Tiwari T (Centers for Disease Control and Prevention (CDC), National Center for Immunization and Respiratory Diseases). Tetanus. Roush SW, Baldy LM, Kirkconnell Hall. Manual for the Surveillance of Vaccine-Preventable Diseases. Updated October 22, 2024. [Full Text].
Thwaites CL, Beeching NJ, Newton CR. Maternal and neonatal tetanus. Lancet. 2015 Jan 24. 385 (9965):362-70. [QxMD MEDLINE Link]. [Full Text].
Prevots DR. Neonatal tetanus. MMWR Morb Mortal Wkly Rep. Dec 31 1999;48 Suppl:176-7.
Hodowanec A, Bleck TP. Tetanus (Clostridium tetani). Bennett JE, Dolin R, Blaser MJ. Mandell, Douglas, and Bennett's Principles and Practice of Infectious Diseases. 8. Elsevier; 2015. 2: 2757-2762. [Full Text].
World Health Organization. WHO Technical Note: Current recommendations for treatment of tetanus during humanitarian emergencies. January 2010. [Full Text].
Sanford JP. Tetanus--forgotten but not gone. N Engl J Med. 1995 Mar 23. 332(12):812-3. [QxMD MEDLINE Link]. [Full Text].
Yeh FL, Dong M, Yao J, et al. SV2 Mediates Entry of Tetanus Neurotoxin into Central Neurons. PLOS Pathogens. 2010. 6:e1001207. [QxMD MEDLINE Link]. [Full Text].
Tetanus vaccines: WHO position paper, February 2017 - Recommendations. Wkly Epidemiol Rec. 2017 Feb 10. 92:53-76. [QxMD MEDLINE Link]. [Full Text].
Pascual FB, McGinley EL, Zanardi LR, Cortese MM, Murphy TV. Tetanus surveillance--United States, 1998--2000. MMWR Surveill Summ. 2003 Jun 20. 52(3):1-8. [QxMD MEDLINE Link]. [Full Text].
Farnworth E, Roberts A, Rangaraj A, Minhas U, Holloway S, Harding K. Tetanus in patients with chronic wounds – are we aware?. Int. Wound J. 2011 Sep 19. 9:93-99. [QxMD MEDLINE Link]. [Full Text].
Gergen PJ, McQuillan GM, Kiely M, et al. A Population-Based Serologic Survey of Immunity to Tetanus in the United States. N Engl J Med. 1995 Mar 23. 332:761-767. [QxMD MEDLINE Link]. [Full Text].
Rhinesmith E, Fu L. Tetanus Disease, Treatment, Management. Pediatr Rev. 2018 Aug. 39 (8):430-432. [QxMD MEDLINE Link]. [Full Text].
Centers for Disease Control and Prevention (U.S.). Center for Surveillance, Epidemiology, and Laboratory Services. National Notifiable Diseases Surveillance System. Weekly cases* of notifiable diseases, United States, U.S. Territories, and Non-U.S. Residents week ending November 2, 2024 (Week 44) Table 1270 Tetanus. CDC Stacks. Available at https://stacks.cdc.gov/view/cdc/169346. November 7, 2024; Accessed: January 6, 2025.
State School Immunization Requirements and Vaccine Exemption Laws. CDC Public Health Law. Available at https://www.cdc.gov/phlp/docs/school-vaccinations.pdf. February 2022; Accessed: January 9, 2025.
Pingali C, Yankey D, Elam-Evans LD, et al. Vaccination Coverage Among Adolescents Aged 13-17 Years - National Immunization Survey-Teen, United States, 2022. MMWR Morb Mortal Wkly Rep. 2023 Aug 25. 72(34):912-919. [Full Text].
Yen LM, Dao LM, Son LH, et al. Role of quinine in the high mortality of intramuscular injection tetanus. The Lancet. 1994 Sep 17. 344:786-787. [QxMD MEDLINE Link]. [Full Text].
Fetuga BM, Ogunlesi TA, Adekanmbi FA. Risk factors for mortality in neonatal tetanus: a 15-year experience in Sagamu, Nigeria. World J Pediatr. 2010 Feb. 6(1):71-5. [QxMD MEDLINE Link]. [Full Text].
Basu S, Paul DK, Ganguly S, Chandra PK. Risk factors for mortality from neonatal tetanus: 7 years experience in North Bengal, India. Ann Trop Paediatr. 2006 Sep. 26(3):233-9. [QxMD MEDLINE Link]. [Full Text].
Li J, Liu Z, Yu C, Tan K, Gui S, Zhang S, et al. Global epidemiology and burden of tetanus from 1990 to 2019: A systematic analysis for the Global Burden of Disease Study 2019. Int J Infect Dis. 2023 Jul. 132:118-126. [QxMD MEDLINE Link]. [Full Text].
Rushdy AA, White JM, Ramsay ME, Crowcroft NS. Tetanus in England and Wales, 1984-2000. Epidemiol Infect. 2003 Feb. 130(1):71-7. [QxMD MEDLINE Link]. [Full Text].
Tetanus in England: 2022. UK.GOV. Available at https://www.gov.uk/government/publications/tetanus-in-england-annual-reports/tetanus-in-england-2022. June 1, 2023; Accessed: January 6, 2025.
Blencowe H, Cousens S, Mullany LC, Lee AC, Kerber K, Wall S, et al. Clean birth and postnatal care practices to reduce neonatal deaths from sepsis and tetanus: a systematic review and Delphi estimation of mortality effect. BMC Public Health. 2011 Apr 13. 11 Suppl 3:S11. [QxMD MEDLINE Link]. [Full Text].
Jones CE, Yusuf N, Ahmed B, Kassogue M, Wasley A, Kanu FA. Progress Toward Achieving and Sustaining Maternal and Neonatal Tetanus Elimination — Worldwide, 2000–2022. Morbidity and Mortality Weekly Report (MMWR). July 18, 2024. Available at https://www.cdc.gov/mmwr/volumes/73/wr/mm7328a1.htm.
Tiwari TSP, Moro PL, Acosta AM. Tetanus. Centers for Disease Control and Prevention. Available at https://www.cdc.gov/pinkbook/hcp/table-of-contents/chapter-21-tetanus.html. April 25, 2024; Accessed: January 6, 2025.
Apte NM, Karnad DR. Short report: the spatula test: a simple bedside test to diagnose tetanus. Am J Trop Med Hyg. 1995 Oct. 53(4):386-7. [QxMD MEDLINE Link]. [Full Text].
Hassel B. Tetanus: Pathophysiology, Treatment, and the Possibility of Using Botulinum Toxin against Tetanus-Induced Rigidity and Spasms. Toxins. 2013 Jan; 5(1): 73–83. 5:73-83. [QxMD MEDLINE Link]. [Full Text].
Bunch TJ, Thalji MK, Pellikka PA, Aksamit TR. Respiratory failure in tetanus: case report and review of a 25-year experience. Chest. 2002 Oct. 122(4):1488-92. [QxMD MEDLINE Link]. [Full Text].
Karnad D, Gupta V. Intensive Care Management of Severe Tetanus. Indian J Crit Care Med. 2021 May. 25:S155-160. [QxMD MEDLINE Link]. [Full Text].
Trieu HT, Anh NTK, Vuong HNT, et al. Long-term outcome in survivors of neonatal tetanus following specialist intensive care in Vietnam. BMC Infec Dis. 2017 Sep 25. 17:646. [QxMD MEDLINE Link]. [Full Text].
Lin TS, Chen LK, Lin TY, Wen SH, Chen MC, Jan RH. Autonomic dysfunction because of severe tetanus in an unvaccinated child. Pediatr Neonatol. 2011 Jun. 52(3):169-71. [QxMD MEDLINE Link]. [Full Text].
Bush LM, Vazquez-Pertejo MT. Tetanus. Porter RE. The Merck Manual of Diagnosis and Therapy. Rahway, NJ: Merck & Co Inc; Reviewed/Revised January 2023. [Full Text].
Steinegger T, Wiederkehr M, Ludin HP, Roth F. Electromyography as a diagnostic aid in tetanus. Schweiz Med Wochenschr. 1996 Mar 9. 126:379-385. [QxMD MEDLINE Link]. [Full Text].
Mitra RC, Gupta RD, Sack RB. Electrocardiographic changes in tetanus: a serial study. J Indian Med Assoc. 1991 Jun. 89:164-167. [QxMD MEDLINE Link]. [Full Text].
Turillazzi E, Neri M, Pomara C, Riezzo I, Fineschi V. An immunohistochemical study on a tetanus fatal case using toxin fragment C (TTC). Should it be a useful diagnostic tool?. Neuropathology. February 2009. 29:68-71. [QxMD MEDLINE Link]. [Full Text].
[Guideline] CDC. Clinical Guidance for Wound Management to Prevent Tetanus. Centers for Disease Control and Prevention. Available at https://www.cdc.gov/tetanus/hcp/clinical-guidance. August 15, 2024; Accessed: December 15, 2024.
[Guideline] CDC. Clinical Care of Tetanus. Centers for Disease Control and Prevention. Available at https://www.cdc.gov/tetanus/hcp/clinical-care. August 15, 2024; Accessed: December 15, 2024.
Bradley FD, Peter ME. Tracheostomy practice in adults with acute respiratory failure. Critical Care Medicine. October 2012. 40:2890-2896. [QxMD MEDLINE Link]. [Full Text].
Ahmadsyah I, Salim A. Treatment of tetanus: an open study to compare the efficacy of procaine penicillin and metronidazole. Br Med J (Clin Res Ed). 1985 Sep 7. 291(6496):648-50. [QxMD MEDLINE Link]. [Full Text].
Prevention and management of wound infection. World Health Organization. 2013 March 02. Available at https://www.who.int/publications/i/item/prevention-and-management-of-wound-infection.
Petitjeans F, Turc J, Coulet O, Puidupin M, Eve O, Benois A. The use of boluses of propofol for the management of severe tetanus in a child. Trop Doct. 2009 Jan. 39(1):52-3. [QxMD MEDLINE Link]. [Full Text].
Boots RJ, Lipman J, O'Callaghan J, Scott P, Fraser J. The treatment of tetanus with intrathecal baclofen. Anaesth Intensive Care. 2000 Aug. 28(4):438-42. [QxMD MEDLINE Link]. [Full Text].
Engrand N, Guerot E, Rouamba A, Vilain G. The efficacy of intrathecal baclofen in severe tetanus. Anesthesiology. 1999 Jun. 90(6):1773-6. [QxMD MEDLINE Link]. [Full Text].
Thomas RM, Bellamy MC. Tetanus in a subcutaneous drug abuser: ineffectiveness of intrathecal baclofen. Anaesth Intensive Care. 2006 Dec. 34(6):811-5. [QxMD MEDLINE Link]. [Full Text].
Ceneviva GD, Thomas NJ, Kees-Folts D. Magnesium sulfate for control of muscle rigidity and spasms and avoidance of mechanical ventilation in pediatric tetanus. Pediatr Crit Care Med. 2003 Oct. 4(4):480-4. [QxMD MEDLINE Link]. [Full Text].
Thwaites CL, Yen LM, Loan HT, Thuy TT, Thwaites GE, Stepniewska K, et al. Magnesium sulphate for treatment of severe tetanus: a randomised controlled trial. Lancet. 2006 Oct 21. 368(9545):1436-43. [QxMD MEDLINE Link]. [Full Text].
Nepal G, Coghlan MA, Yadav JK, et al. Safety and efficacy of Magnesium Sulfate in the management of Tetanus: A systematic review. Trop Med Int Health. 2021 Oct. 26:1200-1209. [QxMD MEDLINE Link]. [Full Text].
[Guideline] Committee on Infecitous Diseases. Recommended Childhood and Adolescent Immunization Schedule: United States, 2025: Policy Statement. Pediatrics. 2024 Nov 21. 69:77-83. [QxMD MEDLINE Link]. [Full Text].
Low R, Young K, Verani L, et al. Point-of-care testing for tetanus immunity: a systematic review and meta-analysis. Emerg Med J. 2022 Apr 04. 39:771-778. [QxMD MEDLINE Link]. [Full Text].
Minta A, Havers F, Tohme R. Tetanus. CDC Yellow Book 2024. Available at https://wwwnc.cdc.gov/travel/yellowbook/2024/infections-diseases/tetanus. Accessed: January 9, 2025.
Liang JL, Tiwari T, Moro P, Messonnier NE, Reingold A, Sawyer M, et al. Prevention of Pertussis, Tetanus, and Diphtheria with Vaccines in the United States: Recommendations of the Advisory Committee on Immunization Practices (ACIP). MMWR Recomm Rep. 2018 Apr 27. 67 (2):1-44. [QxMD MEDLINE Link]. [Full Text].
Sawyer M, Liang JL, Messonnier N, Clark TA. Updated Recommendations for Use of Tetanus Toxoid, Reduced Diphtheria Toxoid, and Acellular Pertussis Vaccine (Tdap) in Pregnant Women — Advisory Committee on Immunization Practices (ACIP), 2012. MMWR Morb Mortal Wkly Rep. 2013 Feb 22. 62:131-135. [QxMD MEDLINE Link]. [Full Text].
Updated recommendations for use of tetanus toxoid, reduced diphtheria toxoid, and acellular pertussis (Tdap) vaccine in adults aged 65 years and older - Advisory Committee on Immunization Practices (ACIP), 2012. MMWR Morb Mortal Wkly Rep. 2012 Jun 29. 61(25):468-70. [QxMD MEDLINE Link]. [Full Text].
Wodi AP, Issa AN, Moser CA, Cineas S. Advisory Committee on Immunization Practices Recommended Immunization Schedule for Adults Aged 19 Years or Older — United States, 2025. MMWR. January 16, 2025. 74(2):30-33. [Full Text].
Issa AN, Wodi AP, Moser CA, Cineas S. Advisory Committee on Immunization Practices Recommended Immunization Schedule for Children and Adolescents Aged 18 Years or Younger — United States, 2025. MMWR. January 16, 2025. 74(2):26-29. [Full Text].
-
Image from "Number of Tetanus Cases Reported and Average Annual Incidence Rates, by State." Pascual FB, McGinley EL, Zanardi LR, et al: Tetanus surveillance—United States, 1998−2000. MMWR Surveill Summ. 2003 Jun 20;52(3):1-8.
-
Image from "Number of Tetanus Cases Reported, Average Annual Incidence Rates, and Survival Status of Patients, by Age Group." Pascual FB, McGinley EL, Zanardi LR, et al: Tetanus surveillance—United States, 1998−2000. MMWR Surveill Summ. 2003 Jun 20;52(3):1-8.
-
Image from "Number of Tetanus Cases Reported Among Persons With Diabetes or Injection-Drug Use (IDU), by Age Group." Pascual FB, McGinley EL, Zanardi LR, et al: Tetanus surveillance—United States, 1998−2000. MMWR Surveill Summ. 2003 Jun 20;52(3):1-8.
-
Reported number of tetanus cases in the United States from 1947-2023. Image from National Notifiable Disease Surveillance System (NNDSS), Centers for Disease Control and Prevention (CDC).

Author
Joseph M Yabes, Jr, MD, FACP Deputy Director, USAF HIV Medical Evaluation Unit, Associate Program Director, Infectious Disease Fellowhip, Brooke Army Medical Center; Core Faculty, Infectious Disease Fellowship, Chair, Virtual Health Subcommittee, San Antonio Uniformed Services Health Education Consortium (SAUSHEC); Assistant Professor, Department of Medicine, Uniformed Services University of the Health Sciences; Adjunct Assistant Professor, Department of Medicine, University of Texas Health Science Center at San Antonio
Joseph M Yabes, Jr, MD, FACP is a member of the following medical societies: American College of Physicians, Armed Forces Infectious Diseases Society, Infectious Diseases Society of America
Disclosure: Received income in an amount equal to or greater than $250 from: MedPage Today LLC.
Coauthor(s)
Ryan McLaughlin, BS MD Candidate, Uniformed Services University of the Health Sciences School of Medicine
Disclosure: Nothing to disclose.
Chief Editor
Additional Contributors
Keith N Chappell, MD Administrative Chief Resident, Junior Attending Resident, Department of Emergency Medicine, Newark Beth Israel Medical Center
Disclosure: Received salary from Newark Beth Israel Medical Center for employment.
Acknowledgements
Leslie L Barton, MD Professor Emerita of Pediatrics, University of Arizona College of Medicine
Leslie L Barton, MD is a member of the following medical societies: American Academy of Pediatrics, Association of Pediatric Program Directors, Infectious Diseases Society of America, and Pediatric Infectious Diseases Society
Disclosure: Nothing to disclose.
Richard B Brown, MD, FACP Chief, Division of Infectious Diseases, Baystate Medical Center; Professor, Department of Internal Medicine, Tufts University School of Medicine
Richard B Brown, MD, FACP is a member of the following medical societies: Alpha Omega Alpha, American College of Chest Physicians, American College of Physicians, American Medical Association, American Society for Microbiology, Infectious Diseases Society of America, and Massachusetts Medical Society
Disclosure: Nothing to disclose.
Daniel J Dire, MD, FACEP, FAAP, FAAEM Clinical Professor, Department of Emergency Medicine, University of Texas Medical School at Houston; Clinical Professor, Department of Pediatrics, University of Texas Health Sciences Center San Antonio
Daniel J Dire, MD, FACEP, FAAP, FAAEM is a member of the following medical societies: American Academy of Clinical Toxicology, American Academy of Emergency Medicine, American Academy of Pediatrics, American College of Emergency Physicians, and Association of Military Surgeons of the US
Disclosure: Nothing to disclose.
Theodore J Gaeta, DO, MPH, FACEP Clinical Associate Professor, Department of Emergency Medicine, Weill Cornell Medical College; Vice Chairman and Program Director of Emergency Medicine Residency Program, Department of Emergency Medicine, New York Methodist Hospital; Academic Chair, Adjunct Professor, Department of Emergency Medicine, St George's University School of Medicine
Theodore J Gaeta, DO, MPH, FACEP is a member of the following medical societies: Alliance for Clinical Education, American College of Emergency Physicians, Clerkship Directors in Emergency Medicine, Council of Emergency Medicine Residency Directors, New York Academy of Medicine, and Society for Academic Emergency Medicine
Disclosure: Nothing to disclose.
Rosemary Johann-Liang, MD Medical Officer, Infectious Diseases and Pediatrics, Division of Special Pathogens and Immunological Drug Products, Center for Drug Evaluation and Research, Food and Drug Administration
Rosemary Johann-Liang, MD is a member of the following medical societies: American Academy of Pediatrics, American Medical Association, and Infectious Diseases Society of America
Disclosure: Nothing to disclose.
Eleftherios Mylonakis, MD, PhD Assistant Professor of Medicine, Harvard Medical School, Assistant in Medicine, Division of Infectious Disease, Massachusetts General Hospital.
Eleftherios Mylonakis is a member of the following medical societies: American College of Physicians, American Society for Microbiology, and Infectious Diseases Society of America.
Disclosure: Nothing to disclose.
Sonali Ray, MD Resident Physician, Department of Family Practice, Capital Health System, University of Medicine and Dentistry of New Jersey
Disclosure: Nothing to disclose.
Gregory William Rutecki, MD Professor of Medicine, Fellow of The Center for Bioethics and Human Dignity, University of South Alabama College of Medicine
Gregory William Rutecki, MD is a member of the following medical societies: Alpha Omega Alpha, American College of Physicians, American Society of Nephrology, National Kidney Foundation, and Society of General Internal Medicine
Disclosure: Nothing to disclose.
Russell W Steele, MD Head, Division of Pediatric Infectious Diseases, Ochsner Children's Health Center; Clinical Professor, Department of Pediatrics, Tulane University School of Medicine
Russell W Steele, MD is a member of the following medical societies: American Academy of Pediatrics, American Association of Immunologists, American Pediatric Society, American Society for Microbiology, Infectious Diseases Society of America, Louisiana State Medical Society, Pediatric Infectious Diseases Society, Society for Pediatric Research, and Southern Medical Association
Disclosure: Nothing to disclose.
Francisco Talavera, PharmD, PhD Adjunct Assistant Professor, University of Nebraska Medical Center College of Pharmacy; Editor-in-Chief, Medscape Drug Reference
Disclosure: Medscape Salary Employment
Robert W Tolan Jr, MD Chief, Division of Allergy, Immunology and Infectious Diseases, The Children's Hospital at Saint Peter's University Hospital; Clinical Associate Professor of Pediatrics, Drexel University College of Medicine
Robert W Tolan Jr, MD is a member of the following medical societies: American Academy of Pediatrics, American Medical Association, American Society for Microbiology, American Society of Tropical Medicine and Hygiene, Infectious Diseases Society of America, Pediatric Infectious Diseases Society, Phi Beta Kappa, and Physicians for Social Responsibility
Disclosure: Novartis Honoraria Speaking and teaching
Mary L Windle, PharmD Adjunct Associate Professor, University of Nebraska Medical Center College of Pharmacy; Editor-in-Chief, Medscape Drug Reference
Disclosure: Nothing to disclose.